
What Exactly Makes a Drug "Narrow Therapeutic Index"?
Not every medication is considered an NTI drug. To keep things objective, the FDA uses a pharmacometric approach to decide which drugs get the "NTI" label. One of the primary yardsticks is the therapeutic index (TI). In simple terms, the TI is the ratio between the dose that causes toxicity and the dose that produces a therapeutic effect. The FDA generally considers a therapeutic index of 3 or less as the cutoff for NTI classification. If a drug's TI is between 3 and 5, it might still be flagged depending on other factors. Beyond just the numbers, the FDA looks at five specific criteria to determine if a drug needs these special standards:- The difference between the minimum effective dose and the minimum toxic dose is no more than two-fold.
- The gap between the lowest and highest drug concentrations in the therapeutic range is very small (maximum 2-fold difference).
- Patients require routine therapeutic monitoring (like regular blood tests) to keep the drug in the safe zone.
- The drug has low-to-moderate within-subject variability (usually ≤ 30%).
- Doctors often adjust doses in tiny increments, typically less than 20%.
The Shift from Standard Bioequivalence to NTI Rules
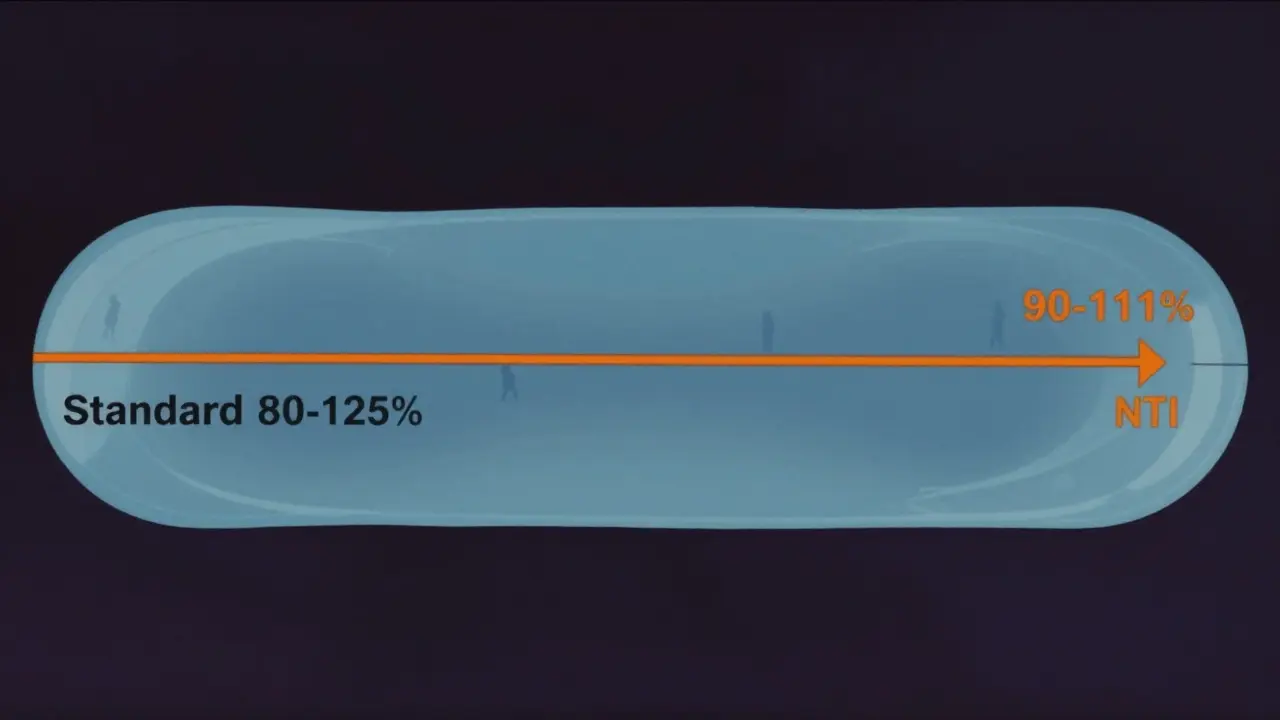
For most generic drugs, the FDA uses a standard bioequivalence range of 80% to 125%. This means that if the generic version delivers the drug into the bloodstream at a rate and extent that falls within this window compared to the brand name, it's usually approved. But for NTI drugs, a 20% difference could be dangerous. Following a pivotal 2010 advisory committee meeting, the FDA shifted gears. They realized that the 80-125% window was far too wide for drugs where precision is everything. Now, they require a much tighter acceptance interval, typically 90.00-111.11%. This ensures that the generic is almost an exact mirror of the brand-name product's performance in the body.Technical Requirements: Scaling and Quality Control
It's not just about the final percentage; the way the FDA tests these drugs is fundamentally different. They use a more nuanced approach called Scaled Average Bioequivalence (SABE). Instead of a one-size-fits-all limit, the FDA scales the limits based on the within-subject variability (WSV) of the reference listed drug. If a drug has moderate variability, it must pass both the reference scaled limits and the traditional 80-125% limits. Additionally, the FDA looks at the ratio of the within-subject standard deviation of the test product to the reference product; the upper limit of the 90% confidence interval must be ≤ 2.5. Quality control at the manufacturing level is also ramped up. While a standard generic might have an assay acceptance range of 90-110%, an NTI generic is held to a tighter 95-105% range. This ensures that the actual amount of active ingredient in each tablet is incredibly consistent.| Requirement | Standard Generic Drug | NTI Generic Drug |
|---|---|---|
| Bioequivalence Range | 80.00% - 125.00% | 90.00% - 111.11% |
| Quality Assay Range | 90% - 110% | 95% - 105% |
| Study Design | Standard BE Study | Replicate Study Designs |
| Variability Approach | Fixed limits | Scaled Average Bioequivalence (SABE) |
Real-World Impact and Clinical Controversies
Does this technical tightening actually work in the real world? The FDA says yes, pointing to evidence that generic NTI drugs are clinically substitutable. For instance, studies on tacrolimus (used in organ transplants) show that generics meet these tighter limits and perform consistently in stable patients. However, not everyone is convinced. There is a long-standing debate, especially regarding antiepileptic drugs. Some clinicians and patients argue that even with the FDA's strict rules, switching from a brand-name antiepileptic to a generic can trigger breakthrough seizures. This conflict often stems from the fact that different patients metabolize these drugs differently, meaning a generic that is "bioequivalent" on average might not be equivalent for every single individual. Because of this, you'll find a strange patchwork of laws. Even though the FDA approves these generics as therapeutically equivalent, some state laws still require a pharmacist to get a patient's explicit consent before substituting an NTI drug, or they may prohibit automatic substitution entirely. The FDA acknowledges this gap and suggests better education for pharmacists to help increase the substitution rate for these safe, approved generics.The Path to Approval for NTI Generics
For a pharmaceutical company, bringing an NTI generic to market is a significantly harder climb than a standard generic. They can't just run a basic study and hope for the best. They must implement replicate study designs, which require larger sample sizes and more complex statistical heavy lifting to prove they hit that narrow 90-111% window. Interestingly, the FDA doesn't actually publish a single, master "NTI Drug List." Instead, they release product-specific guidances. If a manufacturer wants to make a generic version of a specific drug, they have to check the guidance for that particular molecule to see if the NTI requirements apply. This approach allows the FDA to update standards for individual drugs without having to rewrite a massive list every time new data emerges.
Looking Ahead: Global Harmony
Right now, the US is doing things a bit differently than other parts of the world. While agencies like the European Medicines Agency (EMA) and Health Canada generally just tighten the average bioequivalence limits, the FDA's scaled approach is more mathematically complex. Moving forward, the FDA is pushing for "harmonization." The goal is to get global regulatory agencies on the same page so that a drug proven safe and equivalent in the US is viewed the same way in Europe or Canada. As of 2022, about 15% of newly approved generics involve NTI medications, showing that the industry is increasingly capable of meeting these rigorous standards.Why is the 80-125% range not enough for NTI drugs?
In standard drugs, a 20% difference in blood concentration usually doesn't change the clinical outcome. However, for NTI drugs, that same 20% difference can push a patient from a therapeutic level into a toxic level or drop them below the level needed to treat the condition, leading to treatment failure.
Where can I find the official list of FDA NTI drugs?
The FDA does not maintain one single public list. Instead, they provide NTI designations through product-specific guidance documents for each individual medication. Manufacturers must refer to these guidances to determine the specific BE requirements for the drug they are developing.
Are generic NTI drugs actually safe to swap with brand names?
The FDA maintains that generic NTI drugs are therapeutically equivalent and clinically substitutable because they meet much stricter quality and bioequivalence standards (90-111%) than standard generics. However, some clinicians still advise caution with specific drugs like antiepileptics due to individual patient variability.
What is a "replicate study" in the context of NTI drugs?
A replicate study is a specialized bioequivalence design where each subject is given both the test and reference products multiple times in a randomized sequence. This allows researchers to better distinguish between variability caused by the drug formulation itself and variability caused by the individual patient's biology.
How does the FDA's approach differ from the EMA?
The EMA and Health Canada typically use a direct tightening of average bioequivalence limits. The FDA uses a more sophisticated "scaled" approach (SABE), where the limits are adjusted based on the known within-subject variability of the reference drug, providing a more nuanced statistical evaluation.